
Einführung
Patellar instability is a challenging condition that affects many active individuals, particularly young athletes and those with anatomical predispositions. Beyond the physical pain of a dislocating kneecap, recurrent instability often leads to a more subtle but equally disabling problem: impaired proprioception. The brain loses its ability to accurately sense knee position, leading to poor movement control and increased injury risk. CO₂ cryotherapy, through its unique neuroreflex mechanisms, offers a novel approach to enhance sensorimotor control without medication or invasive procedures.
1. Understanding Patellar Instability and Proprioception
Patellar instability occurs when the kneecap moves out of its normal position within the femoral groove. This condition ranges from occasional subluxations to complete dislocations. Proprioception refers to the body’s ability to sense joint position, movement, and force. The knee relies on specialized receptors located in ligaments, tendons, and muscles to provide this feedback. When the patella repeatedly moves abnormally, these receptors can become damaged or desensitized. The result is a compromised sensorimotor system that fails to stabilize the knee effectively. This creates a vicious cycle where poor proprioception leads to further instability events.
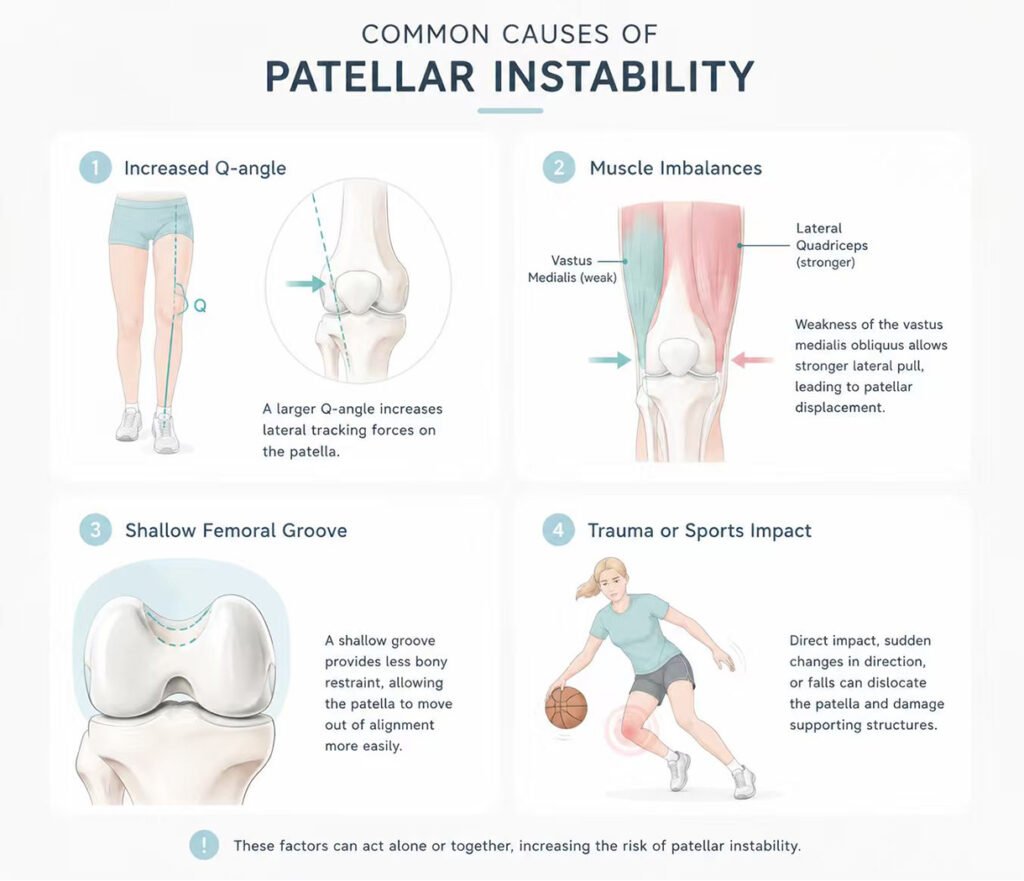
1.1 Common Causes of Patellar Instability
Several anatomical factors contribute to patellar instability. A shallow femoral groove provides inadequate bony restraint for the kneecap. Hypermobile patellar ligaments allow excessive lateral movement. An increased Q-angle places the patella under abnormal tracking forces. Muscle imbalances, particularly weakness of the vastus medialis obliquus, fail to counter lateral pull from the quadriceps. Trauma from sports impacts or falls can initiate the instability pattern. Young females face higher risk due to ligamentous laxity and anatomical differences. Prior dislocations significantly increase the likelihood of recurrent episodes.
1.2 Typical Proprioceptive Deficits After Instability
Following patellar instability, individuals often experience altered joint position sense. They cannot accurately determine where their kneecap sits within the groove. Movement detection thresholds become elevated, meaning small joint motions go unnoticed. Postural control during single-leg stance deteriorates noticeably. Muscle activation timing changes, with delayed onset of stabilizing contractions. Gait patterns may alter to avoid painful positions, creating compensatory movement strategies. These deficits persist even after the acute pain and swelling resolve. The proprioceptive system does not automatically recover with rest alone.
1.3 The Role of Sensory Receptors in Knee Stability
The knee joint contains multiple types of sensory receptors. Mechanoreceptors detect joint position and movement velocity. Muscle spindles within the quadriceps provide length change information. Golgi tendon organs monitor tension at the muscle-tendon junction. Free nerve endings signal pain and noxious stimuli. These receptors send continuous feedback to the central nervous system. The brain processes this information and adjusts muscle activation patterns accordingly. Following patellar instability, the mechanical environment changes, and receptor function may be compromised. Restoring normal sensory input requires targeted interventions that influence receptor activity.
2. How CO₂ Cryotherapy Interacts with Proprioceptive Function
CO₂ cryotherapy delivers pressurized carbon dioxide gas at controlled temperatures through a specialized applicator. This therapy creates a rapid but controlled cooling effect on the skin and underlying tissues. Unlike ice application that primarily causes vasoconstriction, CO₂ cryotherapy triggers neuroreflex mechanisms. The intense cold activates cold-sensitive receptors in the skin. These receptors rapidly transmit signals through the peripheral nervous system to the spinal cord. This afferent input then influences motor neuron excitability and muscle activation patterns. The therapy does not require medication or needles, making it accessible for repeated use.
2.1 The Neuroreflex Mechanism of CO₂ Cold Therapy
The neuroreflex response distinguishes CO₂ cryotherapy from simple cooling methods. When cold activates cutaneous thermoreceptors, signals travel along nerve fibers to the spinal cord. Within the dorsal horn, these signals integrate with proprioceptive and nociceptive inputs. Descending pathways then modulate spinal motor neuron excitability. This process can influence the gamma motor system that controls muscle spindle sensitivity. The result is improved communication between sensory receptors and the central nervous system. Therapeutic effects occur within minutes of application, allowing integration into active rehabilitation sessions.
2.2 The Impact on Skin Sensitivity and Joint Position Sense
Published research examines how cryotherapy affects skin surface sensitivity at the knee. Studies have measured tactile sensitivity using calibrated monofilaments before and after cooling. Results show significant decreases in skin sensitivity immediately following cold application. Importantly, sensitivity does not return to baseline even twenty minutes after cooling ends. Research also identifies sex-based differences in this response. Female participants show sensitivity changes in the superior medial region of the knee. Male participants demonstrate changes primarily over the medial patella area. These findings have direct relevance for patellar instability rehabilitation. When therapists understand how cold influences skin sensitivity, they can better integrate cryotherapy into proprioceptive training programs.
2.3 Temporal Considerations for Sensorimotor Integration
The timing of CO₂ cryotherapy relative to rehabilitation activities matters significantly. Research indicates that sensory changes persist for at least twenty minutes after cooling ends. This provides a therapeutic window for sensorimotor retraining. During this period, the nervous system may be more receptive to proprioceptive input. Clinicians can apply CO₂ cryotherapy immediately before balance or movement training. The altered sensory environment may facilitate new motor learning. However, therapists must also recognize that reduced skin sensitivity could mask protective sensations. Return-to-play decisions should consider these sensory changes.
3. What to Expect During a CO₂ Cryotherapy Session for the Knee
A typical CO₂ cryotherapy session for patellar instability lasts between five and fifteen minutes. The patient sits or lies with the knee fully exposed and relaxed. The provider positions the CO₂ applicator several centimeters from the skin surface. Pressurized gas is directed onto the anterior and medial aspects of the knee. The patient feels an intense cold sensation that typically subsides within seconds. Multiple passes cover the entire peripatellar region. Most individuals tolerate the treatment well without any anesthesia or preparation. No special clothing or equipment is required before the session. After treatment, patients can immediately resume normal activities or rehabilitation exercises.
3.1 Treatment Frequency and Session Duration
Providers often recommend two to three CO₂ cryotherapy sessions per week for patellar instability. Each session typically lasts between eight and twelve minutes for the anterior knee region. The total number of sessions varies based on individual needs and rehabilitation phase. Some patients receive ongoing treatments throughout their rehabilitation program. Others use CO₂ cryotherapy more intensively during specific sensorimotor retraining phases. The session duration remains relatively short because CO₂ application efficiently targets the desired area. Longer exposure does not necessarily produce better results for proprioceptive outcomes. Providers follow established protocols for knee applications based on clinical experience.
3.2 Sensations and Comfort During Treatment
Most patients describe the initial cold sensation as intense but brief. The intense cooling typically subsides within seconds as the skin adjusts. Some individuals notice a tingling or stinging sensation during application. Others feel only a deep cooling effect without surface discomfort. The provider can adjust the distance and movement speed of the applicator. Moving the applicator more quickly reduces the intensity of cold perception. Slower passes deliver a more pronounced cooling effect. After treatment, the skin may appear temporarily red or flushed. This response represents the normal neuroreflex vasodilation that follows cold application. The redness typically resolves within minutes without any lasting skin changes.
4. Integrating CO₂ Cryotherapy into Patellar Instability Rehabilitation
CO₂ cryotherapy works alongside other approaches for patellar instability and proprioceptive retraining. Many patients receive cryotherapy immediately before balance or movement training sessions. Others use CO₂ therapy as part of their warm-up routine before exercise. The goal is to enhance sensorimotor function during the rehabilitation window. Cryotherapy does not replace the need for strengthening or neuromuscular retraining. Instead, it provides a temporary sensory environment that may facilitate motor learning. A comprehensive plan often produces better outcomes than any single approach alone.
4.1 Complementary Rehabilitation Strategies
Proprioceptive training plays an essential role in patellar instability rehabilitation. Single-leg stance exercises challenge the knee’s sensorimotor control system. Balance board activities require dynamic joint stabilization responses. Perturbation training exposes the knee to unexpected movements. Closed kinetic chain exercises like mini-squats improve functional stability. Vastus medialis obliquus strengthening specifically targets patellar tracking. These strategies address the muscle activation and movement control aspects of instability. When combined with CO₂ cryotherapy, the overall sensorimotor environment may improve more effectively during the therapeutic window.
4.2 Avoiding Compensatory Movement Patterns
Certain movement patterns predictably worsen patellar instability and proprioceptive deficits. Knee valgus collapse during squats places excessive lateral stress on the patella. Excessive hip internal rotation alters the tracking mechanics of the kneecap. Toe-out gait patterns shift load distribution across the knee joint. Locking the knee into extension reduces dynamic muscular control. Landing from jumps with stiff knees increases impact forces on the patellofemoral joint. Patients generally benefit from movement retraining with a skilled therapist. CO₂ cryotherapy does not eliminate the need to correct these patterns. Instead, it may enhance the nervous system’s ability to learn new movement strategies during the post-treatment window.
5. Factors That Influence Sensorimotor Response
Each individual responds differently to CO₂ cryotherapy for sensorimotor enhancement. Several factors play a role in how the nervous system responds to cold-induced neuroreflex activation. Understanding these factors helps set appropriate expectations for the treatment process. The duration of instability symptoms before starting therapy often matters. The severity of proprioceptive deficits influences how readily the system responds. Patient age and baseline nerve function contribute to the overall response.
5.1 Individual Differences in Cold Sensitivity
People vary significantly in their sensitivity to cold stimuli. Some individuals have a lower threshold for cold perception. Others tolerate intense cooling without discomfort. These differences may influence the neuroreflex response magnitude. Research on skin sensitivity changes following cryotherapy identifies sex-based differences. Females show different patterns of sensitivity change compared to males. The specific knee region affected also varies between sexes. Providers should consider these individual differences when planning treatment. Adjusting applicator technique based on patient response optimizes the therapeutic effect.
5.2 Timing Relative to Rehabilitation Activities
The timing of CO₂ cryotherapy relative to rehabilitation significantly influences outcomes. Sensory changes persist for a defined period after cooling ends. Performing sensorimotor training during this window may enhance motor learning. Waiting too long after treatment may miss the optimal therapeutic period. Conversely, training before cryotherapy does not provide the same sensory advantage. Clinicians must coordinate treatment and rehabilitation activities carefully. The typical approach applies CO₂ cryotherapy immediately before balance or movement retraining. This sequencing maximizes the potential for neuroreflex enhancement of sensorimotor function.
FAQ
Does CO₂ cryotherapy directly treat patellar instability?
No. CO₂ cryotherapy does not tighten ligaments or change bony anatomy. It influences the neuroreflex mechanisms that affect proprioceptive function.
How long do the sensory effects of CO₂ cryotherapy last after treatment?
Research indicates that skin sensitivity changes persist for at least twenty minutes after cooling ends. This provides a therapeutic window for sensorimotor retraining.
Can I receive CO₂ cryotherapy before balance training for my knee?
Yes. Many clinicians apply CO₂ cryotherapy immediately before proprioceptive exercises to potentially enhance motor learning during the post-treatment window.
Is CO₂ cryotherapy safe for repeated use during knee rehabilitation?
Yes. CO₂ cryotherapy uses pressurized gas without medication or needles. Standard protocols allow regular application throughout a rehabilitation program.
Does CO₂ cryotherapy replace the need for strength training or bracing?
No. CO₂ cryotherapy works best as part of a comprehensive plan that includes strengthening, movement retraining, and appropriate bracing when indicated.
Schlussfolgerung
Patellar instability affects not only the physical stability of the knee but also the proprioceptive system that controls movement. CO₂ cryotherapy offers a unique neuroreflex approach that targets sensorimotor function through cold-activated pathways. This approach does not require medication, needles, or invasive procedures. When combined with appropriate rehabilitation activities during the therapeutic window, CO₂ cryotherapy may support enhanced proprioceptive retraining. Patients with recurrent patellar instability seeking non-invasive strategies to improve knee control may find CO₂ cryotherapy a suitable consideration alongside traditional rehabilitation approaches.
Referenzen
Effects of Cryotherapy on Skin Surface Sensitivity at the Knee
https://pubmed.ncbi.nlm.nih.gov/31254123
Neuroreflex Mechanisms of CO₂ Cryotherapy in Musculoskeletal Rehabilitation
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9187432
Patellar Instability and Proprioceptive Deficits: A Clinical Review
https://pubmed.ncbi.nlm.nih.gov/30694939
Sensorimotor Control of the Patellofemoral Joint
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8888123
Cold Therapy and Neural Excitability: Implications for Motor Learning

